Science Seen Physicist and Time One author Colin Gillespie helps you understand your world.

Herd immunity—friend or enemy?
We can find a way out of the COVID-19 isolation trap.
Herd immunity. What is it? What can it do for us? Or to us?
It can be our best friend and our worst enemy.
The starting point to understanding herd immunity is: It is not about me; it is about us. It is math, pure and relatively simple to understand. Understanding what it is may prove helpful—and even reassuring—in these uncertain times.
Scientists who study a virus determine a number that reflects how easy it is to catch. Let’s call that number R0 (that’s one of the names scientists use). If I catch a virus, I may in turn infect many people . . . or a few . . . or maybe none. So, let’s track some people who have it and see how many other people catch it from them.
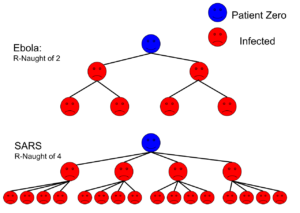 Then we divide the total number of people who caught the virus from them by the total number of people who gave it to them. That number—the average number of people infected by a typical infectious person—is the R0 (also known as the basic reproduction number) of that virus.
Then we divide the total number of people who caught the virus from them by the total number of people who gave it to them. That number—the average number of people infected by a typical infectious person—is the R0 (also known as the basic reproduction number) of that virus.
Experts are working
This kind of tracking is easier said than done. All over the world, experts are working night and day to pin down the new coronavirus’s R0 amid many practical difficulties. The best overview I’ve found is in a March 30 report from a team of 61 epidemiologists in England. Collecting data from eleven European countries they find R0 numbers that are “all over the map” — figuratively speaking.
Their best estimate of R0 for the new coronavirus is about three. Higher R0 means more infectious: For example, measles is horribly infectious with an R0 of about eighteen. Lower R0 means less infectious and a virus with R0 of one or less is not infectious enough to cause a pandemic.
Next key thing to understand is: COVID-19’s high R0 is our enemy; but it can lead us to a friend. What matters is the actual value of R (also known as reproduction number) where we live at any given time. This value is called Rt .
Why does it matter?
The reason that this matters is: Wherever we live, our local Rt can be made lower than the bug’s R0 , depending on what we do, like physical distancing or lockdown.
The last key thing to understand is: When we reduce COVID-19’s Rt to a number less than one, it cannot maintain a local epidemic (let alone a pandemic—a new worldwide epidemic) even if it has a high R0 . It’s simple: If everyone who gets the bug infects less than one other person, the epidemic is dying out instead of increasing and will soon be gone.
That’s what all this staying home and physical distancing is about: getting our Rt below one. Once we do this, the epidemic is on its way to ending—but only if we keep on staying home and distancing.
Another way to reduce COVID-19’s Rt
However, there is another way to reduce COVID-19’s Rt to a number less than one; and it’s a way that does not depend on staying home or distancing: If two-thirds of any given population is immune, its Rt is one.
Here is the explanation: If on average each person who gets the bug “infects” three people—but two of those three are immune—only one of those three gets the bug and only that one is then able to infect others.
This is called herd immunity. It is not a property of “me”; it is a state of “us” (the herd) and that infection.

In general, we have herd immunity to any infectious disease when all but a fraction of the population (one divided by R0 ) has immunity to it. Right now, for us this is a BIG DEAL: This new virus has a not-too-large R0 so we need only some (i.e., about two-thirds) of us to become immune, a relatively achievable target, to stop the wave of infection. And keeping it stopped does not require us to keep on distancing.
Of course, herd immunity does not descend upon us suddenly when that mathematical average hits exactly one point zero. The virus becomes less infectious as Rt becomes closer to one.
So how can Rt be made to decrease? In just two ways. One way is natural: Those who get (and survive) the virus will gain a degree of immunity. The other way is artificial: Vaccination.
We will achieve herd immunity
Thing is, either way we will achieve herd immunity regardless of what we do. The key questions are: How long will we take to achieve it and what will it cost us in lives and economic damage along the way? Both the delay and the damage will depend on what we do.
And there’s the rub (thankyou Shakespeare): Developing, testing and producing a vaccine plus vaccinating billions of people would take years. In practical terms, this is unlikely to happen. One way or another, we will have moved on, just as we did after SARS.
This is where we should be careful what we wish for. Right now, we just want to slow the spread (reduce Rt ) so that critical care in hospitals is not overwhelmed. We are enduring draconian measures to achieve this: Anything to stop the virus! But, once success is in view people will want to relax those draconian measures. What then?
It appears that for the early and for-now-suppressed outbreak in China, only a modest fraction of its population was infected. And in Europe this fraction may be less than ten percent to date. So only modest progress is being made toward herd immunity. As each country moves to restart its economy, its epidemic may come back—perhaps more overwhelmingly.
Is a likely-losing gamble our only alternative to economic ruin while we wait for a vaccine that will arrive too late, if ever?
Another path
Indeed, there is another path we could choose: As gamer Marty Brenner pointed out a few days ago, the virus is a vaccine.
Here’s the deal, for healthy volunteers only:
- Get infected (a small controlled dose; small dose means lower risk).
- Get monitored, with free access to health care.
- Get treated when a treatment becomes available, if needed.
- Get better, mostly (but maybe not all) with mild if any symptoms.
- Get tested for immunity (a different test, more below).
- Get an International Vaccination Certificate and photo “Certified Immune” ID.
- Get $1,000 for your time and trouble (far cheaper than current crisis programs).
- Get back to work.
It will be controversial but this “thread-the-needle” faster approach toward herd immunity could get the economy going at optimal speed while ensuring local health care systems are not threatened. If done well, fewer should die than would otherwise.
It will need a new test (one that is simpler, faster and cheaper than the PCR test that sees if you have the virus). A serological test, now under urgent development, basically will see if you had the virus and so have acquired immunity.
Expect new tests soon, as well as approved treatments and a growing conversation about our way forward.
In sum, we are coming to a three-way fork in our road:
- We can stay locked down waiting for a vaccine that will not arrive in time;
- We can go back to work with some precautions praying the bug won’t come back; or
- We can offer controlled infection to volunteers who almost all recover and go back to work.
I’m in line for the third way.
Image Credits:
Kiera Campbell, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=79523883
Vaccines: Their Risk, Safety, and Effectiveness; https://vaccine-risks.com/natural-herd-immunity/
I actually though of this idea… but went a step further. The US, for example, has 5 million empty hotel rooms.
The program would work by admitting screened, low-risk group volunteers to be exposed… then chill in the hotel until recovered… so that we’re building Herd Immunity rapidly without collateral spread. The hospitals stay underwhelmed, Herd Immunity grows between 1-2 orders of magnitude faster, the volunteers are getting the best care/monitoring… and are moved to the hospital for the cases that require it.
Unfortunately. You do not mention the death rate at all in your article. Do you think it is morally right to sacrifice 1-2% of the population to achieve herd immunity , actually the number will be higher because of the people who cannot access ICUs in hospitals when they need them weather they have COVID-19 or not. That number will be higher than mortality rate of COVID-19.
As for using the virus as a vaccine that will not work, because so many people and some are young without underlying conditions died because of the virus. Unless there is an effective treatment or at medication that helps with prophylaxis exposure, using the virus as a vaccine will not work. Even giving an experimental vaccine then exposing someone to the virus is controversial and has ethical problems.
What is more important, money or human life. You can never bring anyone back from the dead, but the economy will recover, it could be a year, two , three, 10 or more. But it will.
Is your suggestion still hypothetical or is this actually something you can sign up to do? I would gladly become infected (and quarantine of course) in order to not infect loved ones unknowingly at a later date.
Colin, please tell me if viruses sometimes mutate in a friendly direction, i.e. don’t make you sick anymore. The problem may be that we then might not know about their existence. Maybe some viruses already do /have done this.
The spherically shaped Coronavirus looks quite charming anyway.
I like your reasoning and your math but do wonder if the considerable number of infected people who remain asymptomatic also find a home in your theory. They will of course form part of the herd.
Option 3 ignores the element of mutation. The virus mutates all the time (my reading pegs it at 1/3 to 1/2 that of influenza), and every infection is an opportunity for further mutation. So far research is not showing any sign that the mutations are going to change the course of the pandemic, and hopefully we keep it that way. At the moment we have a disease that should be effectively wiped out with a single vaccine. Option 3 however risks developing mutations that will change the course of the pandemic, requiring multiple vaccines to target multiple strains – or worse yet it becomes an on-going seasonal disease with annual vaccinations like flu. While it looks like SARS-CoV-2 will remain genetically stable and be wiped out, we shouldn’t be giving it extra opportunities to become worse than it already is.
The science and math aspect is logical and reassuring. But what I find even more reassuring is you have presented (in my opinion anyways) a sensible, informed and consensual alternative to our currently accepted alternatives. I don’t like feeling like a defenceless sitting duck. Being engaged and informed is good for the mind/soul, and I think can only help us move forward.
Thank you for helping us make sense of our current state of affairs.
I agree in the 3rd option. Although it does depend on when the quick testing to see if people have had the virus and have developed immunity to the virus becomes available. Then we would just have to isolate the vulnerable or ones that weren’t infected till hers immunity has been reached. Otherwise were stuck with the loosening of guidelines with a more dangerous outcome if the virus comes back again 2x.
Rather than recruiting sacrificial heroes to be infected couldn’t a partial loosening of physical distancing requirements achieve the same result, herd immunity? Isn’t this where we are likely headed, that after the first onslaught of the virus is tempered by physical distancing, our leaders will allow or encourage us to return to slightly more risk exposure, such as going to work, but wearing masks and continuing to disinfect and maintain distance most of the time? I know, easier said than done, a fine balancing act that we may not have enough knowledge and experience to pull off very well. But I think we will be forced in that direction by simple economic necessity and will have to learn by trial and error. Immunity testing is clearly required in any case, as you say.
You are quite right, Jeremy. Loosening will do it. But actually, THAT is the sacrificial lamb approach and the lmbs don’t get to choose. Live infection should only proceed if level-4 labs like the National Microbiology Laboratory in Winnipeg can produce controlled low doses of live virus; and these result in mild or even symptom-free infections. It may well be possible to inoculate a million Canadians for example, with zero deaths and few serious cases. The uncontrolled dose approach will not be as kind to those same people. Thanks for your insightful comment.
According to your virus spread math we would need to achieve immunity among 70% of 38 million Canadians = 26 million or so. Let’s say that about 10% of Canadians, or 4 million become immune without being intentionally infected/immunized, this leaves another 21 million to be intentionally infected – a tall order. How long would that take? Would it actually be faster than a gradual loosening of physical distancing?
My other question is whether we can be sure that the intentional infection process would actually result in immunity? When public health people have been asked to comment on whether people who have had the virus are immune, they have hedged and said they think so but can’t be certain. I guess this question will be resolved eventually through wide testing and better data.
You and your family could volunteer first.
Actually, Walter, if you check the end of the article, you’ll see I already did. But my spouse disputes my claim to first priority. As volunteering should be the safest (see my reply to Jeremy Hull) as well as best-lifestyle and most-profitable option, this is in fact a very selfish choice. Your comment may have been tongue-in-cheek; my wish to be early in the queue is serious.
Thanks anyway and I offer you a story in fair trade:
The late eminent Australian virologist, Dr. Eric French, was my godfather. In the 1957, he was the first to isolate a flu virus. He cultured it in eggs (as scientists still do today). From this culture the first flu vaccine was then made.
Years later, Eric’s daughter married my brother. I had occasion to chat with her only the other day.
She said she thought making the vaccine was quick, maybe two months, but then (lacking today’s rules and tests) its safety may have seemed to be in doubt.
Her father (she informed me) was sure it was safe, and safer than not having it. He publicly inoculated himself, his wife, his daughter, then 11 or 12, and his even younger son.
The Asian flu killed about a million people worldwide before the vaccine came into full effect.